Insights
Low Energy, Brain Fog, and Low Drive: Is Hormone Imbalance the Cause? What Tallahassee Adults Need to Know

You used to bounce out of bed. Now getting up feels like a negotiation. Your thoughts that were once sharp take longer to land. Work that used to come easily now requires twice the effort for half the output. Your drive — professional, creative, physical, sexual — has quietly downshifted without any clear reason why.
Most adults in this situation do the same thing: they push through it, assume it is stress, and wait for life to settle down. Then a year passes. Then two. And it still does not settle.
For a significant number of adults across Tallahassee, these symptoms are not about stress or schedule. They are about hormones. Specifically, about a gradual hormonal shift that most providers never screen for unless the patient asks directly — and that responds well to medically supervised treatment when identified early.
Here is what hormone replacement therapy in Tallahassee at an integrated practice looks like when it starts with the right questions.
Why Hormone Imbalance Is Chronically Under-Identified
Hormones are the body's messaging system. Estrogen, progesterone, testosterone, cortisol, insulin, thyroid hormone, and DHEA collectively regulate energy metabolism, sleep architecture, mood stability, cognitive speed, libido, muscle maintenance, immune function, and inflammatory response. When any part of that system drifts out of range, the downstream effects are broad, slow-moving, and easy to attribute to something else.
According to the Endocrine Society, hormonal changes typically develop gradually over months or years — which is precisely why most patients spend a long time searching for an explanation before a clinical evaluation surfaces the actual cause.
The problem compounds because hormone symptoms overlap heavily with other common conditions. Fatigue, brain fog, weight gain, low mood, and reduced drive are also symptoms of depression, sleep apnea, iron deficiency, B12 deficiency, thyroid dysfunction, and chronic stress. Standard primary care panels frequently miss sex hormone imbalances because they are not included in a routine metabolic or CBC workup unless specifically ordered.
Patients who go years without identification are not being failed by a broken system. They are navigating a system that was not designed to look at hormones proactively. An integrated practice with a dedicated hormone-optimization provider — like University Physical Medicine in Tallahassee — fills that gap.
The Symptom Clusters That Point to a Hormone Problem
Hormone symptoms rarely appear in isolation. They cluster. And the specific pattern of clustering often points to which hormone system is most affected. Below are the most diagnostically significant groupings seen in clinical practice.
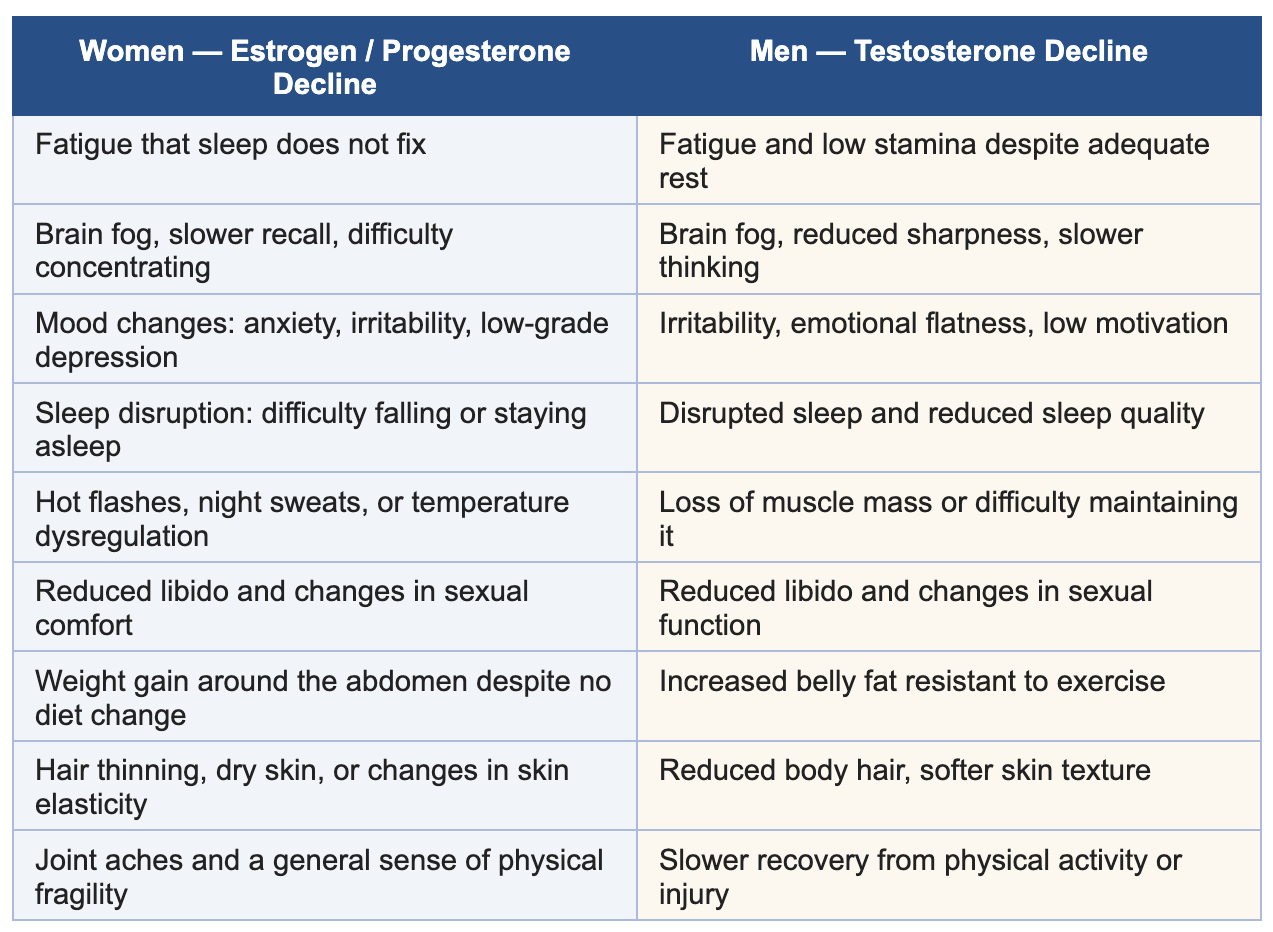
A key clinical pattern worth noting: when three or more symptoms from either column are present simultaneously and have persisted for more than three months, a comprehensive hormone panel is warranted. Symptom clusters are far more diagnostically meaningful than any single symptom in isolation.
The Thyroid Factor Most People Miss
Any clinical conversation about low energy and brain fog that does not evaluate thyroid function is incomplete. Hypothyroidism — underactive thyroid — produces a symptom profile that closely mirrors sex hormone imbalance: fatigue, cognitive slowing, weight gain, cold sensitivity, hair thinning, depression, and reduced drive.
According to the Mayo Clinic, hypothyroidism affects an estimated 1 in 300 people in the United States, with women significantly more affected than men — and subclinical hypothyroidism (where TSH is elevated but within an extended normal range) is considerably more prevalent and frequently missed on standard panels that test TSH alone without free T3 or free T4.
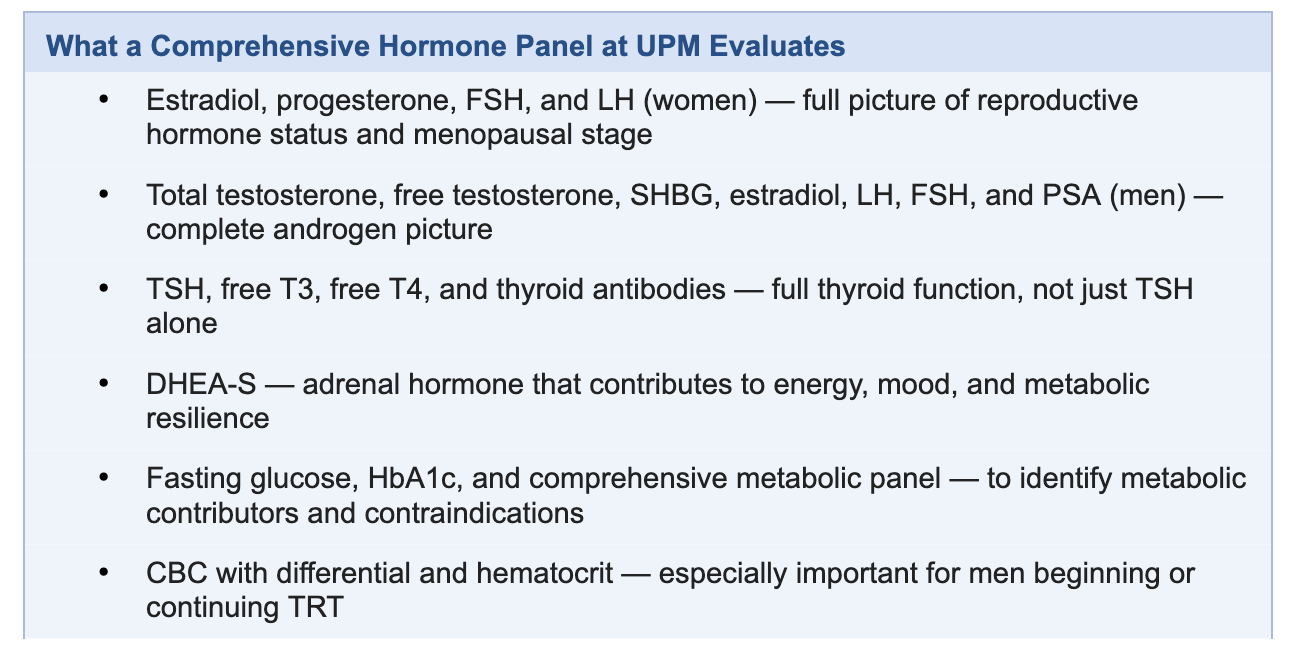
At University Physical Medicine, Celeste Lind, A.R.N.P. evaluates thyroid function as a standard component of the hormone workup — not as an afterthought. A panel that includes TSH, free T3, free T4, and thyroid antibodies gives a complete picture rather than the partial one that a TSH-only screen provides. In many patients, optimizing thyroid function alongside sex hormone levels produces meaningfully better outcomes than addressing either in isolation.
What Medically Supervised Hormone Treatment Looks Like in Tallahassee
HRT for Women
For women in perimenopause or menopause whose lab work confirms a clinically significant estrogen or progesterone decline, medically supervised HRT for women in Tallahassee can meaningfully reduce hot flashes, restore sleep quality, stabilize mood, protect bone density, and return cognitive sharpness. BioTE pellet therapy, for which Celeste Lind is a certified provider, delivers consistent sustained hormone release without the daily fluctuation of creams, pills, or patches.
The American College of Obstetricians and Gynecologists (ACOG) supports hormone therapy for symptomatic menopausal women without significant contraindications, noting that benefits for most women in early menopause outweigh risks when treatment is appropriately individualized. Compounded and pellet-based hormone preparations are not FDA-approved pharmaceutical products in the traditional sense, and an informed-consent conversation about available evidence, delivery options, and personal risk factors is a required part of the process at UPM before any treatment begins.
TRT for Men
For men whose lab work confirms low total and free testosterone alongside matching symptoms, testosterone replacement therapy in Tallahassee is managed as a supervised medical protocol — not a quick prescription. Baseline labs, monitored follow-up panels at regular intervals, and ongoing symptom assessment are built into every patient's plan from day one.
According to MedlinePlus (NIH), testosterone levels in men decline at roughly one to two percent per year after age 30. By the mid-forties, many men have experienced a 20 to 30 percent reduction from peak levels — a shift that is clinically significant but routinely unscreened. TRT at UPM includes a proactive conversation about risks including potential fertility impact, hematocrit elevation, and cardiovascular considerations before any treatment is initiated.
Peptide Therapy
For patients seeking optimization beyond foundational hormone restoration, peptide therapy in Tallahassee offers an additional layer of medically supervised support. Peptides are short-chain amino acid sequences that function as signaling molecules — directing specific biological processes including cellular repair, growth hormone release, inflammatory modulation, sleep quality, and metabolic function.
At UPM, peptide protocols are prescribed within a broader clinical context — not as standalone supplements or internet-order products. Specific peptide selection, dosing, and monitoring are individualized to the patient's lab findings, symptom profile, and treatment goals. The research base for peptide therapy is still expanding, and Celeste Lind discusses realistic expectations, evidence levels, and monitoring requirements openly with every patient before beginning a protocol.
Why Symptoms Alone Are Never Enough to Start Treatment
A symptom checklist can open a conversation. It cannot close a clinical decision.
Fatigue, brain fog, and low drive are genuinely non-specific. Starting hormone therapy based on symptoms alone — without lab confirmation of what is actually elevated, depressed, or out of ratio — risks treating the wrong problem, undertreating the right one, or missing a contributing condition that would have changed the approach entirely.
At UPM, no hormone treatment plan is proposed before a comprehensive panel is reviewed. The evaluation process protects the patient from unnecessary treatment and from the kind of under-evaluation that produces a prescription without a diagnosis. Patients who invest in the right workup first consistently report better outcomes, fewer side effects, and more confidence in the plan they are following.
What Makes UPM's Approach Different in Tallahassee
Most patients who arrive at University Physical Medicine for a hormone consultation have already been told their labs are "normal." Many of them are right to be skeptical. Reference ranges on standard panels are population averages — they identify disease, not optimization. A testosterone level at the bottom quartile of the normal range is technically within range, but it is not the level at which most men feel or function optimally.
Celeste Lind, A.R.N.P. brings close to 40 years of clinical experience — beginning as an EMT and paramedic, through FSU nursing training, family practice, and eventually a focus on hormone optimization, BioTE certification, and medically supervised vitality care. That depth of clinical experience means patients are evaluated as individuals, not processed through a protocol.
The integrated structure of UPM means that a patient whose low energy has both a hormonal component and a structural or sleep-disruption component can address both within the same practice — with Dr. Belletto and Celeste Lind collaborating on a unified care plan rather than the patient coordinating between separate providers who have never spoken to each other.
Frequently Asked Questions
Q: How do I know if my brain fog and fatigue are hormonal or just stress?
A: Stress-related fatigue typically fluctuates with external circumstances and improves during periods of reduced pressure. Hormone-related fatigue tends to be persistent, present regardless of how much you sleep or rest, and accompanied by a cluster of other physical and cognitive changes. A comprehensive lab panel is the only reliable way to distinguish the two — symptoms alone cannot make that determination.
Q: What is the difference between HRT and TRT?
A: Hormone replacement therapy (HRT) is a broader term typically used to describe estrogen, progesterone, or combined hormone supplementation in women — particularly in the context of perimenopause and menopause. Testosterone replacement therapy (TRT) refers specifically to testosterone supplementation, most commonly used in men with clinically confirmed low testosterone, though testosterone also plays a role in women's hormone health and is sometimes included in female hormone protocols at lower doses.
Q: Are bioidentical hormones safer than synthetic hormones?
A: The term "bioidentical" refers to hormones that are chemically identical in structure to those produced by the human body — not to a regulatory approval status or a safety classification. Compounded bioidentical hormones are not FDA-approved pharmaceutical products in the traditional drug approval sense, and they have not undergone the same clinical trial process as branded pharmaceutical hormones. Decisions between compounded and pharmaceutical options should be made on the basis of individual clinical need, available evidence, and a full informed-consent discussion — not on marketing language. Celeste Lind discusses these distinctions openly at every hormone consultation.
Q: How is peptide therapy different from hormone therapy?
A: Hormones are signaling molecules that bind to specific receptors and trigger broad systemic effects. Peptides are shorter amino acid chains that act more specifically — directing targeted processes like growth hormone release, cellular repair, inflammatory modulation, or metabolic function. The two are not interchangeable, and they are often used together in a complementary way. Both require a clinical evaluation and ongoing monitoring to be used safely and appropriately.
Q: How long before I feel a difference on hormone therapy?
A: Most patients begin noticing changes in energy, mood, and sleep quality within four to six weeks of correctly dosed hormone therapy. Cognitive improvements often become more apparent at the eight to twelve week mark. Full effects on body composition and physical performance typically take three to six months. Individual response varies considerably based on the degree of imbalance, the delivery method, and whether other contributing factors such as thyroid function or sleep quality are also being optimized.
Start With the Right Workup — Not a Guess
Low energy, brain fog, and lost drive are not inevitable parts of getting older. For many Tallahassee adults, they are measurable, addressable physiological changes that respond to the right clinical approach.
Celeste Lind, A.R.N.P. and the University Physical Medicine team start every hormone consultation with a comprehensive lab panel and a full clinical picture — not a symptom checklist and a protocol. If you have been told your labs are normal but still do not feel right, that conversation is worth having.
Schedule your hormone consultation today or call (850) 576-2129 to speak with our team.
University Physical Medicine | 1224 Ocala Rd, Tallahassee, FL 32304
Mon / Wed / Thu: 8:30 AM – 5:30 PM | Tue / Fri: 8:30 AM – 12:30 PM
Medical Disclaimer: This article is for general informational purposes only and does not constitute medical advice, diagnosis, or treatment. Hormone therapy decisions are individualized and require a clinical evaluation, comprehensive lab work, and a full review of personal health history and risk factors by a licensed healthcare provider. Always consult your provider before beginning, stopping, or modifying any hormone-related treatment plan.


