Insights
Migraine Relief Center Tips: Why Your Neck Is the Cause

You know the pattern. A dull ache starts behind one eye or at the base of your skull. Within an hour it has climbed into a full migraine — light sensitivity, nausea, the kind of pain that forces you into a dark room and costs you the rest of the day. You wait it out, take something for it, and eventually it passes.
Then it comes back. Same pattern, same location, often the same trigger. You've tried tracking your diet, managing your sleep, cutting your screen time. And still, every few weeks, it finds you again.
If that sounds familiar, our Migraine Relief Center at University Physical Medicine in Tallahassee may have the piece you've been missing. What most patients — and many general practitioners — have never screened for is this: the upper neck is one of the most significant and treatable contributors to recurring migraines. Not the only cause. But a structural and neurological piece that, in a meaningful share of patients, has never been evaluated.
Here is what the research shows, what cervicogenic headache actually means, and why migraine treatment in Tallahassee at an integrated chiropractic practice may offer something most patients have never been offered before.
How Many People Are Living With Recurring Migraines
Migraine is not a minor inconvenience. According to the American Migraine Foundation. more than 39 million people in the United States live with migraine. It ranks as the third most common illness worldwide and the sixth most disabling. In Florida, it affects roughly 12 to 15 percent of adults, with women affected at three times the rate of men.
Despite how common it is, migraine stays undertreated. Most patients rely on acute medications — triptans, NSAIDs, or over-the-counter combinations — without ever getting a plan designed to reduce how often attacks happen. Medication addresses the event. Standard migraine care rarely asks why the attacks keep coming.
According to Florida Health, Leon County. neurological conditions including chronic headache disorders cut into quality of life and workplace output across the Tallahassee metro area. Non-pharmacological, cause-directed care for recurring headaches is a real gap for most patients here.
The Cervicogenic Connection — What Most Patients Are Never Told
The upper cervical spine — the joints, muscles, and nerve structures at C1, C2, and C3 — shares neurological territory with the trigeminal nerve system. That system is the primary pain-signaling pathway for headaches. Dysfunction in the upper neck, from joint restriction, muscular tension, disc changes, or postural load, can feed into the same central pain pathways that drive migraine attacks.
This overlap happens at the trigeminocervical nucleus — a region in the brainstem where signals from the upper cervical nerve roots and the trigeminal nerve meet. Research published in the Journal of Orthopaedic and Sports Physical Therapy found that cervical musculoskeletal dysfunction is measurably present in a significant share of migraine patients — including reduced cervical range of motion, upper trapezius trigger point activity, and upper cervical joint stiffness — compared to headache-free controls.
When cervical dysfunction and migraine occur together, two things happen. The neck dysfunction contributes a direct sensitizing input into the trigeminocervical nucleus, lowering the threshold for a full migraine attack. It also produces its own headache pattern — cervicogenic headache — that patients and providers often mistake for migraine because the symptoms overlap so closely.
Migraine vs. Cervicogenic Headache: The Overlap That Causes Confusion
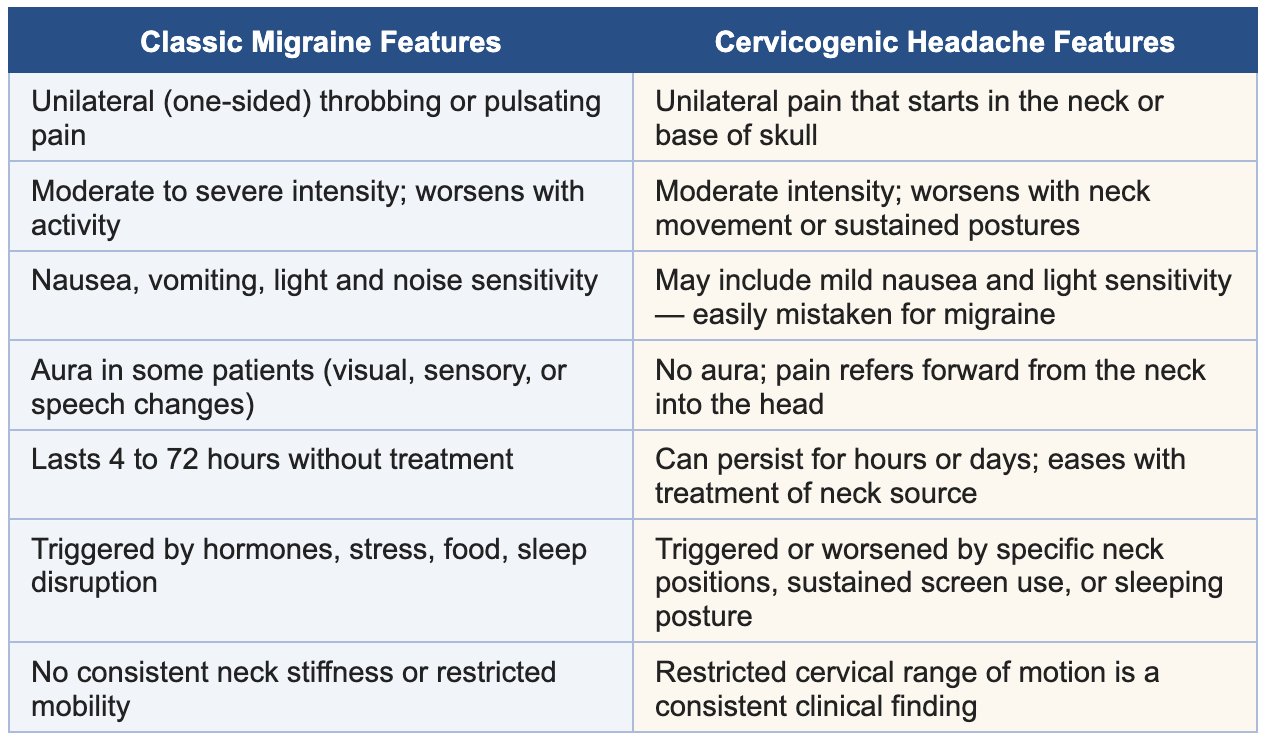
Many patients with recurrent migraines also have a cervicogenic component that has never been identified. When both are present, treating only the migraine with medication while the cervical dysfunction goes unaddressed is one of the most common reasons attacks keep coming back at the same rate regardless of pharmaceutical management.
Why the Neck Goes Unexamined in Most Migraine Workups
Standard migraine management follows a neurological path. A patient presents with recurring headaches, gets a clinical history review and possibly an MRI to rule out secondary causes, and leaves with a preventive or abortive medication plan. Physical examination of the cervical spine — joint mobility, muscle palpation, postural review, upper cervical provocation testing — almost never happens in a neurology or primary care headache workup.
That's not a criticism of neurology. Neurologists evaluate and manage neurological pain pathways. Cervical joint dysfunction, upper trapezius trigger points, and forward head posture patterns fall outside that scope. That evaluation belongs within chiropractic and integrated musculoskeletal assessment.
For Tallahassee migraine patients who've been on the same medication for years with the same attack frequency, a cervical evaluation by an experienced chiropractor for migraines in Tallahassee is often the first time anyone has physically examined the structures that may be keeping the problem alive. Our Migraine Relief Center starts there.
What a Cervical Assessment for Migraines Looks Like at UPM
A cervical evaluation for migraine patients at University Physical Medicine is built to answer specific clinical questions. It's not a replacement for neurology. The evaluation includes:
- Cervical range of motion testing: Quantifying restriction in flexion, extension, rotation, and lateral flexion. Upper cervical restriction is consistently present in cervicogenic headache and often in mixed presentations.
- Upper cervical joint provocation: Manual palpation and segmental assessment of C1, C2, and C3 joint mobility and pain reproduction — the clinical finding that distinguishes cervicogenic from purely vascular or neurological headache.
- Muscle and trigger point assessment: Palpation of the suboccipital muscles, upper trapezius, sternocleidomastoid, and levator scapulae for active trigger points that refer pain into the head and lower migraine threshold.
- Postural and kinetic chain review: Forward head posture and thoracic mobility assessment. For every inch the head shifts forward from neutral, the effective load on the cervical spine rises substantially — a pattern common in Tallahassee's state and university workforce.
- Headache history and pattern mapping: Location, onset, duration, triggers, and response to position change. When mapped against the physical findings, these details determine whether a cervical component is present and how large its contribution is likely to be.
What Chiropractic Care for Migraines Actually Involves
Chiropractic care for cervicogenic or mixed migraine presentations isn't a single adjustment and a hope. A structured care plan includes:
Upper Cervical Spinal Manipulation
Targeted manipulation of the upper cervical joints — C1, C2, and C3 — restores segmental mobility and reduces the sensitizing input these restricted joints send into the trigeminocervical nucleus. A 2017 randomized controlled trial in the European Journal of Pain found that spinal manipulative therapy at the cervical level produced statistically significant reductions in migraine frequency and intensity compared to control groups over 16 weeks.
Soft-Tissue and Trigger Point Work
Active trigger points in the suboccipital and upper trapezius muscles are among the most consistent drivers of referred head pain and reduced migraine threshold. Manual soft-tissue release, dry needling where available, and myofascial techniques directed at these muscles reduce the peripheral sensitization that feeds centrally into migraine pathways.
Postural Rehabilitation and Cervical Strengthening
Restoring deep cervical flexor strength and thoracic mobility allows the head to sit in neutral rather than forward of the center of gravity. That reduces sustained mechanical load on the structures driving cervicogenic sensitization. Without a rehab component, manual treatment produces shorter windows of relief because the postural mechanics haven't changed.
Adjunct Therapies
For patients with significant soft-tissue involvement or chronic muscular tension around the neck and shoulders, shockwave therapy and Class IV laser therapy can reduce trigger point activity and tissue inflammation that manual treatment alone may not fully clear. Therapeutic ultrasound and muscle stimulation are also used when clinically indicated.
What Chiropractic Care for Migraines Cannot Do
An honest clinical team draws a clear line here. Chiropractic care is not a cure for migraine. Migraine is a complex neurological condition with a strong genetic component, a range of established triggers, and a well-documented vascular and neurological mechanism that medication addresses effectively in many patients.
For patients whose migraines have a meaningful cervicogenic component — which clinical research suggests is a substantial subset — addressing the cervical dysfunction can reduce attack frequency, reduce intensity, and in some cases significantly extend the time between episodes. For patients whose migraines are primarily hormonal or vascular with no significant cervical component, the cervical assessment will show that clearly, and appropriate referral or co-management follows.
The goal of neck pain and migraine care at University Physical Medicine is to identify what's actually driving your specific recurrence pattern — and address it directly rather than assuming the answer before the evaluation is done. That's what our Migraine Relief Center is designed to do.
Frequently Asked Questions
Q: Can a chiropractor actually help with migraines?
A: For patients whose migraines have a cervicogenic component — meaning upper cervical joint dysfunction or muscular trigger points are contributing to migraine sensitization — chiropractic care has a meaningful evidence base for reducing attack frequency and intensity. Multiple randomized controlled trials have documented clinically significant improvements in migraine patients receiving spinal manipulative therapy targeting the cervical spine. Whether chiropractic fits your specific presentation requires a cervical evaluation and headache history review.
Q: How do I know if my migraines have a neck component?
A: Several patterns suggest cervical involvement: headaches that consistently start at the base of the skull before spreading forward; pain that worsens with sustained neck positions like looking at a screen for hours; restricted cervical range of motion; tenderness at the upper cervical joints or suboccipital muscles. A structured clinical exam is the most reliable way to find out.
Q: What is cervicogenic headache and how is it different from migraine?
A: Cervicogenic headache originates from dysfunction in the cervical spine — joints, muscles, or discs — and refers pain into the head via the shared neurological territory of the trigeminocervical nucleus. Unlike migraine, it's consistently linked to neck movement and posture, doesn't include aura, and is reliably reproduced by palpation of the upper cervical joints. Many patients have both at once, which is why a physical cervical exam alongside a headache history review matters for accurate differentiation.
Q: Will I need to stop my migraine medication to try chiropractic care?
A: No — and any clinical team suggesting otherwise should be approached with caution. Chiropractic care for cervicogenic migraine contribution works alongside appropriate neurological and pharmaceutical management, not instead of it. The goal is to address the structural component while your existing medical management stays in place. Medication changes are decisions made between you and your prescribing provider.
Q: How many visits does it typically take to notice a reduction in migraine frequency?
A: Most patients with a clear cervicogenic component notice changes in headache frequency or intensity within four to eight weeks of consistent cervical care and postural rehab. Recurrent migraine with a long history of cervical dysfunction typically requires both an active treatment phase and a maintenance phase to hold the improvement. The structural changes that took years to develop don't fully resolve in a few sessions.
Your Neck Deserves to Be Part of the Conversation
If your migraines keep coming back on the same schedule regardless of what you try, something hasn't been evaluated yet. University Physical Medicine's clinical team in Tallahassee performs structured cervical assessments for migraine patients that most headache sufferers have never received — and builds care plans around what the findings actually show.
Dr. Belletto and the UPM team see new patients at 1224 Ocala Rd — one mile from FSU and TCC — with same-day appointments typically available.
Schedule your cervical evaluation today or call (850) 576-2129 to speak with our team directly.


